What Is ARFID? Understanding Avoidant/Restrictive Food Intake Disorder


- ARFID is more than picky eating. It’s a real eating disorder that can affect nutrition, growth, and day-to-day life, even though it’s separate from body image concerns.
- The difference between picky eating and ARFID comes down to impact. When eating habits become so limited that they affect health, social life, or development, it’s time to take a closer look.
- ARFID can show up in different ways, including low appetite, strong sensory aversions, or fear of things like choking or vomiting.
- ARFID can affect people of any age or body size. It’s driven by real physical and psychological factors, including sensory sensitivity, past experiences, and how the brain processes food.
- With the right support, recovery is absolutely possible. Treatment works best with a team approach, combining medical care, nutrition support, and therapy to help expand food variety and reduce anxiety around eating.

Avoidant/restrictive food intake disorder (ARFID) is an eating disorder where someone eats a very limited amount or variety of food (or both). Unlike with most other eating disorders, these symptoms don’t show up because of body image or weight concerns. Instead, they are due to factors like low appetite, sensory sensitivities, or fear of negative food-related experiences like choking or vomiting. ARFID can affect kids, teens, and adults, and over time, it can take a real toll on physical health, emotional well-being, and everyday life.
The good news: With the right, evidence-based support, those with ARFID can expand their diet, reduce anxiety around food, and build a more flexible, nourishing relationship with eating.
Read on to learn what ARFID is, what causes it, common symptoms to look for, how it’s diagnosed, and how treatment works.
What is ARFID?
Avoidant/restrictive food intake disorder (ARFID) is an eating disorder. But unlike many other eating disorders, body image or weight concerns are not the main driver here. ARFID is typically diagnosed when someone consistently eats too little food, too narrow a range of foods, or both, in a way that affects their nutrition, health, and/or daily life.
In real life, that might look like relying on a short list of “safe” foods, avoiding entire food groups, or struggling to eat enough to meet basic needs. Under the surface, these patterns are driven by underlying factors—like how someone experiences hunger, sensory input, or fear—but what you tend to see day to day is a very limited range of foods, avoiding certain meals or situations, or feeling anxious around eating (we’ll break this down more below).
ARFID is most commonly diagnosed in children and is often thought of as a childhood condition. And much of the research we have focuses on kids and teens—estimates suggest that anywhere from 0.3% to 15.5% of children and adolescents meet criteria for ARFID.
But it can affect people of any age and body size. While there’s far less research on adults, what we do have suggests that ARFID affects roughly 0.3% of the general population.
Indeed, while it often begins in childhood, ARFID can persist into adulthood. It can even show up later in life: For instance, after a stressful or frightening food experience (like choking or getting sick).
ARFID is a relatively new diagnosis, only appearing in the DSM since 2013, so it’s still lesser known than many other eating disorders, and many providers aren’t as knowledgeable about it. This can contribute to people going undiagnosed—especially adults, since the common misconception is that ARFID only affects kids. And while it’s not as widely recognized as other eating disorders, ARFID is more common than many people realize—some studies estimate that as many as 15.5% of people will experience ARFID.
It also doesn’t have a specific “look.” Someone can be underweight, at a typical weight, or in a larger body and still be dealing with ARFID. What matters is how much their eating patterns are impacting their health and their life.
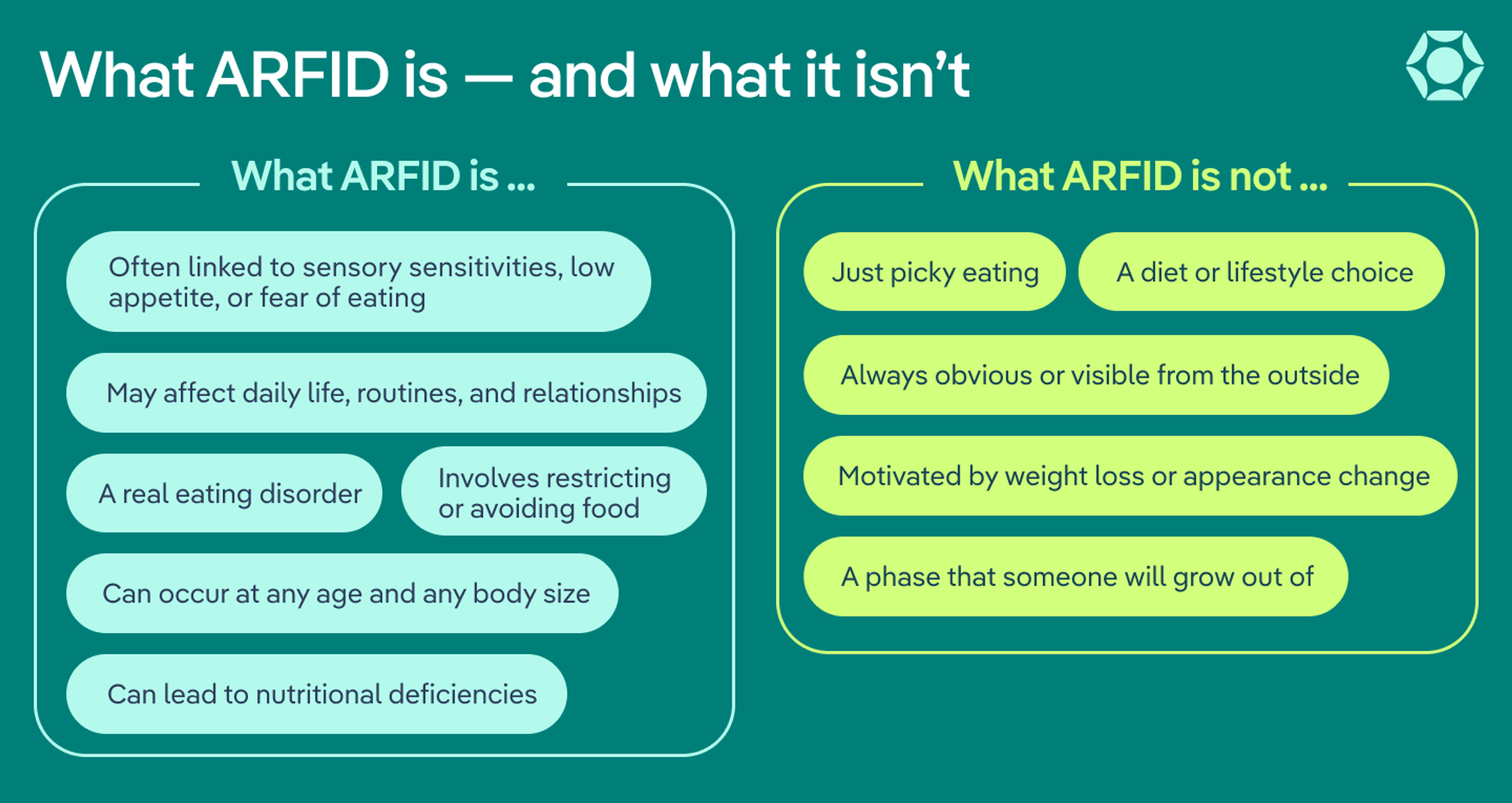
What ARFID Is — and What It Isn’t
What ARFID is
- A real eating disorder
- The restriction or avoidance of food
- Influenced by sensory sensitivities, low appetite, or fear of eating
- A cause of nutritional deficiencies
- An influence on daily life, routines, and relationships
- A disorder that affects any age and any body size
What ARFID is NOT
- A diet or lifestyle choice
- Just picky eating
- Driven by a desire to lose weight or change appearance
- Always obvious or visible from the outside
- A phase that someone will grow out of
What are the three subtypes of ARFID?
ARFID Subtypes at a Glance
ARFID presentation | What it can look like | Example |
Lack of interest in eating | Low appetite or little interest in food or eating | Often forgets to eat or feels full after just a few bites |
Sensory sensitivity | Avoids foods with certain tastes, textures, smells, colors, or temperatures | Only eats foods with a specific texture (like crunchy or smooth) |
Fear of adverse consequences | Avoids food due to fear of choking, vomiting, allergic reactions, or getting sick | Stops eating certain foods—or solid foods altogether—usually after a traumatic incident, like choking or vomiting |
ARFID doesn’t look the same for everyone. Clinicians often group it into three main “presentations,” but these aren’t rigid categories. Many people experience a mix of presentations, and symptoms can shift over time. Here are the three types of ARFID.
Lack of interest in food and low appetite
Some people with ARFID simply don’t feel very interested in food. They may forget to eat, feel full quickly, or find eating more like a chore than something enjoyable. Meals might get skipped without much thought, or a few bites may feel like enough.
In some cases, this pattern starts early in life, with ongoing feeding challenges or low hunger cues. It can also be influenced by other factors, like certain medical conditions or medications. For example, some people with ADHD struggle to notice hunger signals, and stimulant medications can further reduce appetite.
Selective eating due to sensory sensitivity
For others, the issue isn’t how much they eat—it’s what they can tolerate eating. Strong sensitivities to texture, smell, taste, temperature, or even how a food looks can make many foods feel overwhelming or “unsafe.”
This can lead to a very short list of acceptable foods, often ones that feel predictable and consistent (like specific brands, plain foods, or foods prepared in a very particular way. Small changes (like a different texture or brand) can make a food suddenly feel impossible to eat.
This kind of sensory sensitivity is common in people with ARFID who are also on the autism spectrum, though it can affect anyone.
Avoiding eating due to fear of an adverse outcome
In this presentation, eating is tied to fear. Someone may worry that eating will lead to choking, vomiting, an allergic reaction, or another painful or distressing experience.
Often, this is triggered by a specific event, like choking or getting food poisoning. Other times, the fear builds gradually. Either way, the result is the same: avoiding more and more foods, or eating less overall, to try to stay “safe.” Severe cases of this food aversion disorder can lead to significant weight loss or medical complications.
What are the symptoms of ARFID?
It’s not always easy to tell when eating habits have crossed the line from “picky” into something more serious. A helpful benchmark to remember: If someone’s eating is starting to affect their physical health, emotional well-being, or ability to live their day-to-day life, there is likely a problem.
Below are some common ARFID symptoms and warning signs to look out for.
Physical symptoms
- Low weight or noticeable weight loss
- Faltering growth in children or teens
- Nutritional deficiencies
- Dizziness or lightheadedness
- Stomach cramps
- Constipation
- Irregular menstrual cycles
- Delayed puberty in preteens
Behavioral symptoms
- Difficulty concentrating
- Sleep problems
- Lethargy
- Social withdrawal
- Irritability
Food-related symptoms
- A general lack of interest in food and eating
- Not enjoying eating, finding eating to be a chore, or feeling like eating is not worth the effort
- Being highly sensitive to specific characteristics of foods (like texture, smell, or taste) and avoiding foods with those characteristics
- A small list of “acceptable” or “safe” foods that gets smaller over time
- Fear of something bad happening after eating, such as choking, vomiting, or having an allergic reaction
- Rigid habits or rituals around eating (eating foods in a certain order, keeping foods a certain distance from one another)
- Lack of appetite
- Anxiety around mealtimes
Anxiety and fear in particular often play a significant role in ARFID. Someone with ARFID might be nervous to eat and become extremely upset or worked up around mealtimes, especially if new or challenging foods are on the table. “This might look like anything from a lot of arguing with their loved one to having a full-blown tantrum,” says Jessie Menzel, PhD, vice president of clinical programs at Equip.
Warning signs
Beyond the symptoms above, these broader warning signs can help you spot when something more serious may be going on. Keep an eye out for these behaviors or situations:
- Regularly feeling stressful or tense around meals
- Avoiding social situations because of food (like restaurants, events, or eating at others’ homes)
- Being willing to eat only in very specific settings or when food is prepared a certain way
- Eating a shrinking list of foods over time.
- Cutting out entire food groups
- Noticing that eating feels harder than it should
- Exhibiting increasing rigidity around brands, preparation, or who makes the food
- Plateauing growth in children (height or weight not increasing as expected)
Ultimately, Menzel emphasizes the importance of trusting your gut. If eating feels harder than it should—for you or your loved one—that’s a sign it’s time to seek support.
How is ARFID diagnosed?
ARFID is diagnosed by a qualified healthcare professional—like a physician, psychologist, or psychiatrist who is particularly knowledgeable about ARFID—often as part of a broader, team-based evaluation. You can start by taking a simple self-screening as a first step.
Clinicians first look at how someone’s eating patterns are affecting their health and daily life. This can include things like weight changes, nutritional deficiencies, reliance on supplements, or difficulty participating in school, work, or social situations.
Providers also look closely at what’s driving the restriction and rule out other possible explanations. This includes determining whether eating patterns are related to body image or a desire to lose weight (which would point to a different eating disorder), or whether they’re better explained by a medical condition or another mental health diagnosis.
If those causes don’t fully explain what’s going on, providers consider whether the pattern fits ARFID—where restriction is driven by things like low appetite, sensory sensitivities, or fear around eating.
In younger children, clinicians may also consider pediatric feeding disorder (PFD) as a diagnosis. This is a condition that can look similar to ARFID, but is related to development/skills-based factors rather than psychological factors. PFD includes feeding difficulties related to medical, developmental, or skill-based challenges. An ARFID diagnosis, on the other hand, is a mental health condition specifically tied to patterns of food avoidance or restriction without body image concerns.
Because ARFID can show up in different ways, it’s important to understand the full picture so you or your loved one can get the right support.
What are the health risks of ARFID?
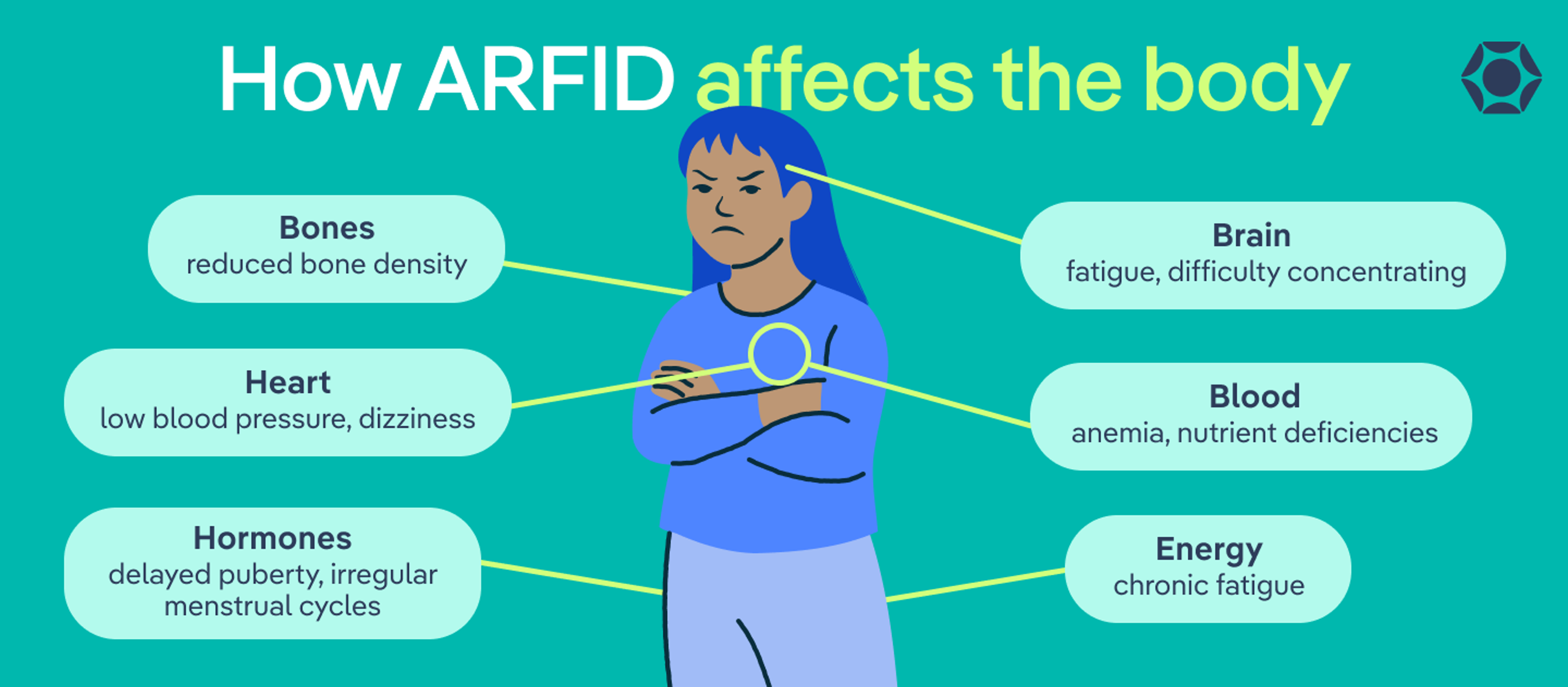
How ARFID Affects the Body
- Brain: fatigue, difficulty concentrating
- Heart: low blood pressure, dizziness
- Bones: reduced bone density
- Blood: anemia, nutrient deficiencies
- Hormones: delayed puberty, irregular menstrual cycles
- Energy: chronic fatigue
ARFID can impact the entire body. When someone isn’t getting enough calories, nutrients, or variety in their diet, multiple body systems can be affected. How severe those effects are depends on how restrictive the eating pattern is and how long it’s been going on.
It’s also important to remember that these risks aren’t always obvious right away, and someone doesn’t have to look visibly underweight to be struggling. Even subtle or gradual changes in eating can have real effects on the body over time, which is why early support and treatment matter.
Potential health complications of ARFID include:
- Malnutrition
- Dehydration
- Electrolyte imbalances
- Anemia
- Low blood pressure
- Bone loss or reduced bone density
- Delayed puberty
- Poor growth in children
- Fatigue or low energy
- Social isolation
What are the causes and risk factors of ARFID?
At this time, there’s no single, clear-cut cause of avoidant/restrictive food intake disorder. Like most eating disorders, ARFID tends to develop from a mix of biological, psychological, and environmental factors, and that mix looks different from person to person.
Some factors that may contribute to the development of ARFID include:
- A family history of eating disorders
- Sensory processing differences (for example, heightened sensitivity to taste, texture, or smell)
- Neurodivergence, such as ADHD or autism
- Differences in how the brain regulates appetite and hunger cues
- Anxiety disorders or high baseline anxiety
- A traumatic food-related experience, such as choking, vomiting, or a severe allergic reaction
ARFID vs. picky eating: what’s the difference?
“This is the number one question I get from parents and other providers,” says Menzel. And for good reason—on the surface, picky eating and ARFID can look very similar.
The difference comes down to severity and impact.
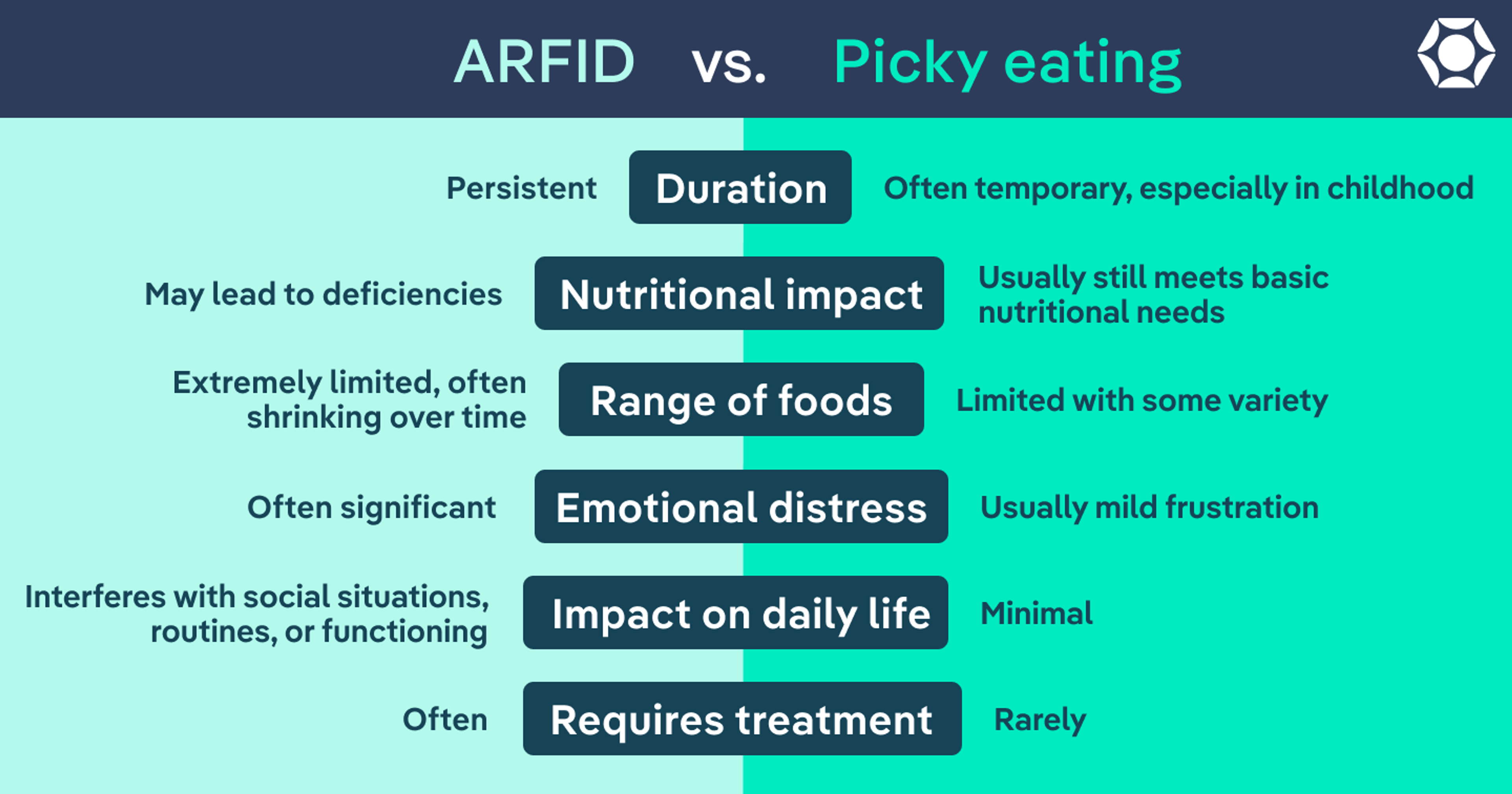
Feature | ARFID | Picky eating |
Duration | Persistent | Often temporary, especially in childhood |
Nutritional impact | May lead to deficiencies | Usually still meets basic nutritional needs |
Range of foods | Extremely limited, often shrinking over time | Limited with some variety |
Emotional distress | Often significant | Usually mild frustration |
Impact on daily life | Interferes with social situations, routines, or functioning | Minimal |
Requires treatment | Often requires professional support | Rarely requires treatment |
Picky eating is common, especially in childhood. And while it can be frustrating, it usually doesn’t affect someone’s health or daily life.
What sets ARFID apart is “the extent to which they narrow what they eat and the persistence with which they narrow,” explains Menzel.
With ARFID, eating patterns are more extreme and don’t tend to improve over time. The range of foods a person eats may continue to shrink, and that restriction can start to affect multiple areas of life. For example:
- Nutritional needs aren’t being met, or there’s a risk of deficiencies.
- Eating interferes with school, work, or social life (like skipping lunch, avoiding birthday parties, or feeling unable to eat at restaurants).
- Meals become a major source of stress or conflict.
- In children, growth (height or weight) may slow or plateau.
Flexibility is another key difference. Someone with picky eating may have preferences, but they can usually adapt when needed, like trying something new at a restaurant or when eating at a friend’s house.
With ARFID, that flexibility is much lower. According to Menzel, someone may only eat a specific food prepared in a very specific way and not tolerate even small changes. Over time, that rigidity can make everyday situations feel overwhelming or even impossible.
What are the best treatments for ARFID?
ARFID is highly treatable, and benefits most from a team-based approach that addresses both the physical and psychological aspects of eating. Here are the most effective treatment strategies.
Medical care
Medical providers help monitor health and make sure the body is getting what it needs to recover. This may include:
- Tracking weight and growth (especially in children)
- Restoring weight
- Identifying and treating nutritional deficiencies
- Monitoring co-occurring conditions (like anxiety, ADHD, or GI issues)
- Managing medications, if needed
Patients may also work with specialists that can help address underlying or co-occurring conditions that could be contributing to ARFID symptoms. These include:
- Gastroenterologists
- Allergists
- Neurologists
- Psychiatrists
Nutritional counseling
Dietitians play a key role in helping people expand what and how much they eat at a pace that feels manageable. Support may include:
- Building balanced, realistic meal plans
- Increasing food variety gradually
- Teaching strategies to manage food anxiety
- Addressing specific challenges like texture sensitivities or fear foods
- Food bridging, where someone starts with a “safe” food and slowly makes small changes (like shape, brand, or preparation) to expand their comfort zone
Therapy
Therapy helps address the underlying drivers of ARFID, like anxiety, fear, or past traumatic experiences with food. Common therapeutic approaches include:
- Family-based treatment for ARFID (FBT-ARFID): Considered the gold standard of care for young people with anorexia nervosa, FBT empowers family members to take a central role in treatment to stop disordered behaviors and nourish their child.
- Cognitive behavioral therapy for ARFID (CBT-AR): This specialized type of CBT involves several phases. First, it focuses on teaching the patient about ARFID and how it manifests. Then, it helps patients notice and challenge the thoughts and behaviors of ARFID.
- Exposure and response prevention (ERP): Food exposures are a central component of ARFID treatment, and this method has been shown to be highly effective. It provides a safe, supportive space for the patient to face challenging or anxiety-provoking foods and experiences. Over time, they gradually become accustomed to and more comfortable with those foods and are able to expand overall food variety. However, it’s important to note that ERP is really only an appropriate treatment approach for individuals with the fear of aversive consequences presentation of ARFID. It unfortunately does not effectively target the other two presentations.
Treatment settings
Treatment can happen in different settings depending on the level and type of support a person needs. Common options include:
- Outpatient care: This involves regular sessions with a therapist, dietitian, and/or medical provider while continuing daily life.
- Intensive outpatient or day programs: These offer more structured support with multiple sessions per week, usually involving at least one meal at the program during each session.
- Inpatient or residential care: These options provide higher-level support that involves living in a clinical or non-clinical treatment setting and getting 24/7 care. Inpatient hospitalization is generally used to address any acute medical concerns.
- Virtual care: Many levels of care—including outpatient, IOP, and PHP—can now be delivered virtually. This allows individuals to receive structured, multidisciplinary support from home. For people with ARFID who are medically stable, virtual programs (like Equip) can be an effective option across a range of severity levels.
How to find professional help
ARFID is highly treatable, but it’s important to get the right support from a team of ARFID-informed specialists. A pediatrician or primary care provider is often a good place to start, however, many general providers are not knowledgeable about ARFID, so if yours is not, seek out an expert, like those at Equip—the largest ARFID treatment provider in the country—to talk through your concerns and next steps.
When evaluating providers or treatment options, look for:
- A multidisciplinary team (medical, nutrition, and mental health support)
- Experience treating ARFID specifically—not just eating disorders in general
- A treatment plan that addresses both nutrition and the psychological side of eating
Once you’ve booked an initial appointment, a little prep can go a long way. Taking these steps beforehand can help ensure a productive conversation:
- Write down symptoms or changes you’ve noticed
- Track patterns (foods avoided, mealtime stress, weight or growth changes)
- Bring questions about the treatment approach and what to expect next
How to support your loved one through recovery
If someone you love is showing signs of ARFID, it’s important to know this: it’s not your fault, and it’s not theirs. Eating disorders aren’t a choice. With the right support, recovery is possible, and getting connected with experienced professionals is the first step.
Once your loved one is in treatment, here are a few ways you can support them:
- Be patient: Progress can be slow, especially at the beginning. It may feel like a lot of effort for small changes, but those small wins matter and add up over time, according to Menzel.
- Stay open to what progress looks like: Someone with a very limited diet isn’t going to suddenly love every food. Try to let go of specific expectations and focus on gradual progress instead.
- Create a non-judgmental environment: Your loved one’s experience with food may be very different from yours. Reactions like pressure, frustration, or surprise can backfire. What helps most is supporting their willingness to explore, not whether they like a food right away.
- Build a support system: ARFID can feel isolating, especially if it’s new to you. Connecting with others—whether through support groups or mentorship—can make a big difference for both you and your loved one.
The bottom line
ARFID is more than just picky eating. It’s an eating disorder that can make food feel stressful, overwhelming, or even scary—and it can impact health and daily life in real ways.
It doesn’t look exactly the same for everyone. For one person, it might mean eating the same few foods every day. For others, it might look like avoiding restaurants and social events or skipping meals without realizing it. None of it is a choice or something someone just “grows out of.”
The good news: With the right support, people really do get better. Over time, eating can feel easier, less stressful, and a lot more flexible.
Frequently asked questions (FAQs)
What is the difference between ARFID and picky eating?
Picky eating is common (especially in childhood) and usually doesn’t affect health or daily life. People may have preferences, but they can still meet their nutritional needs and adapt in different situations. ARFID is more severe and persistent, and people affected tend to eat a much narrower (and often shrinking) range of foods that can lead to nutritional deficiencies, anxiety around eating, social avoidance, and, in children, stunted or delayed growth.
What are the health risks of ARFID?
ARFID can affect multiple body systems over time. Possible risks include malnutrition, dehydration, fatigue, dizziness, nutrient deficiencies, low bone density, delayed puberty, and social isolation.
Can adults have ARFID?
Yes. While ARFID often begins in childhood, it can continue into adulthood or develop later in life. This is especially common after a stressful or traumatic food-related experience (like choking or food poisoning).
Learn more about ARFID
Looking to go deeper? These resources can help you better understand how ARFID shows up and what effective support can look like:
- ARFID in children (coming soon)
- ARFID screener
- ARFID in adults
- ARFID symptoms
- ARFID causes (coming soon)
- Types of ARFID
- ARFID treatment
- What is ARFID?
- How Equip is leading treatment
Deep dive recommendations
If you want to learn more or find additional support, these trusted resources can help:
- Equip: In-depth articles, treatment information, and support options
- Feeding Matters: Resources on feeding challenges, including ARFID and pediatric feeding disorder
- F.E.A.S.T. (Families Empowered and Supporting Treatment of Eating Disorders): Guidance and support for families
- National Eating Disorders Association (NEDA): Education, screening tools, and support resources
James, Rachel Marie et al. “Physical health complications in children and young people with avoidant restrictive food intake disorder (ARFID): a systematic review and meta-analysis.” BMJ paediatrics open vol. 8,1 e002595. 8 Jul. 2024, doi:10.1136/bmjpo-2024-002595
Kambanis, P Evelyna, and Jennifer J Thomas. “Assessment and Treatment of Avoidant/Restrictive Food Intake Disorder.” Current psychiatry reports vol. 25,2 (2023): 53-64. doi:10.1007/s11920-022-01404-6
Kaşak, Meryem et al. “Selective Eating and Sensory Sensitivity in Children With ADHD: A Comparative Study of ARFID Symptom Profiles.” The International journal of eating disorders vol. 58,10 (2025): 1991-2002. doi:10.1002/eat.24512
Ramirez, Zerimar, and Sasidhar Gunturu. “Avoidant Restrictive Food Intake Disorder.” PubMed, StatPearls Publishing, 2024, www.ncbi.nlm.nih.gov/books/NBK603710/.
Riaz, Yumna, and Consolato Sergi. “Feeding Disability in Children.” PubMed, StatPearls Publishing, 2022, www.ncbi.nlm.nih.gov/books/NBK564306/.
Rosania, Kimberly, and James Lock. “Family-Based Treatment for a Preadolescent With Avoidant/Restrictive Food Intake Disorder With Sensory Sensitivity: A Case Report.” Frontiers in psychiatry vol. 11 350. 8 May. 2020, doi:10.3389/fpsyt.2020.00350
Sanchez-Cerezo, Javier et al. “What do we know about the epidemiology of avoidant/restrictive food intake disorder in children and adolescents? A systematic review of the literature.” European eating disorders review : the journal of the Eating Disorders Association vol. 31,2 (2023): 226-246. doi:10.1002/erv.2964
Seetharaman, Sujatha, and Errol L Fields. “Avoidant/Restrictive Food Intake Disorder.” Pediatrics in review vol. 41,12 (2020): 613-622. doi:10.1542/pir.2019-0133
Menzel, Jessie E, and Taylor R Perry. “Avoidant/Restrictive Food Intake Disorder: Review and Recent Advances.” Focus (American Psychiatric Publishing) vol. 22,3 (2024): 288-300. doi:10.1176/appi.focus.20240008
Norris, Mark L et al. “Building evidence for the use of descriptive subtypes in youth with avoidant restrictive food intake disorder.” The International journal of eating disorders vol. 51,2 (2018): 170-173. doi:10.1002/eat.22814
Taylor, Caroline M, and Pauline M Emmett. “Picky eating in children: causes and consequences.” The Proceedings of the Nutrition Society vol. 78,2 (2019): 161-169. doi:10.1017/S0029665118002586
Thomas, Jennifer J et al. “Cognitive-behavioral treatment of avoidant/restrictive food intake disorder.” Current opinion in psychiatry vol. 31,6 (2018): 425-430. doi:10.1097/YCO.0000000000000454









